
The medical infrastructure of the United States is rapidly approaching a dangerous breaking point.
For many decades, the nation has heavily relied upon brilliant medical professionals from all over the world to keep its hospitals fully operational.
This international talent pool has been particularly vital for small towns and underserved rural communities that often struggle to attract domestic talent.
However, a newly implemented wave of extremely strict immigration policies has severely fractured this essential medical pipeline..
From shockingly high new visa application fees to overwhelming bureaucratic delays, the current administration’s aggressive border and immigration strategies are sending shockwaves through the medical community.
The harsh reality on the ground is becoming impossible to ignore for hospital administrators and patients alike.
Trump’s immigration policy sidelines foreign doctors right in the middle of a historic medical shortage, directly threatening the quality of patient care across the entire country.
As America continues to grapple with an aging demographic and a domestic medical education system that simply cannot keep up with patient demand, intentionally restricting foreign-born healthcare workers is creating a catastrophic perfect storm.
This highly detailed analysis explores the escalating U.S. physician deficit, the absolutely critical role of International Medical Graduates, and exactly how recent executive orders are leaving hospitals dangerously understaffed.
Understanding the Severe and Growing U.S. Physician Deficit
To truly comprehend the devastating impact of these new immigration rules, one must first look at the extreme fragility of the American healthcare workforce.
The United States is currently staring down the barrel of a massive, unprecedented shortfall of qualified medical professionals.
According to recent extensive studies by the Association of American Medical Colleges, the nation is projected to lack up to 86,000 physicians within the next decade.
This alarming deficit is primarily driven by several unavoidable converging demographic and structural factors that cannot be fixed overnight.
First and foremost is the rapidly aging population of the United States.
The massive generation known as the Baby Boomers is entering its senior years, resulting in millions of Americans who now require far more complex, chronic, and frequent medical attention.
Secondly, the doctors themselves are aging right alongside their patients.
A shockingly high percentage of currently practicing physicians are over the age of sixty and are widely expected to retire within the next five to ten years.
Furthermore, there is a massive bottleneck in the medical residency system that prevents quick solutions.
While enrollment in U.S. medical schools has slowly increased over the years, the number of federally funded residency training slots has remained largely stagnant due to outdated Medicare funding caps established back in the late 1990s.
Because a doctor absolutely cannot practice medicine independently in America without completing a residency, this bottleneck severely limits how fast the country can produce new domestic doctors.
The domestic production line for physicians is simply mathematically incapable of meeting the skyrocketing healthcare demands of the public.
This painful shortage is already being felt most acutely in essential fields like primary care, emergency medicine, psychiatry, and rural family medicine.
These are exactly the specialties where U.S.-trained medical students frequently decline to practice, often opting instead for more lucrative, highly specialized roles in affluent urban centers.
Why International Medical Graduates (IMGs) Are Indispensable
Into this massive, widening gap step the International Medical Graduates, commonly referred to as IMGs.
These are highly skilled foreign nationals who successfully attended rigorous medical schools outside the United States.
They have actively chosen to uproot their lives and move to the U.S. to complete their grueling residency training and dedicate their careers to practicing medicine in American communities.
The raw data surrounding these professionals highlights an undeniable and deep-rooted American dependence on foreign medical talent.
Today, foreign-trained doctors make up an astonishing twenty-five percent of all practicing physicians and surgeons currently operating in the United States.

In foundational medical fields like primary care and internal medicine, that percentage is often significantly higher.
Beyond just the sheer volume of their numbers, IMGs are geographically vital to the survival of the American healthcare landscape.
Recent healthcare data reveals that nearly twenty-one million Americans currently live in specific geographic areas where foreign-trained physicians account for at least half of the entire local doctor workforce.
Because IMGs frequently utilize specific visa waiver programs that legally require them to work in federally designated Health Professional Shortage Areas for several years, they truly serve as the backbone of rural healthcare.
Without the constant influx of these foreign doctors, countless rural health clinics, critical access hospitals, and community health centers would simply be forced to permanently close their doors.
The Crippling Financial Burden of the New H-1B Visa Fee
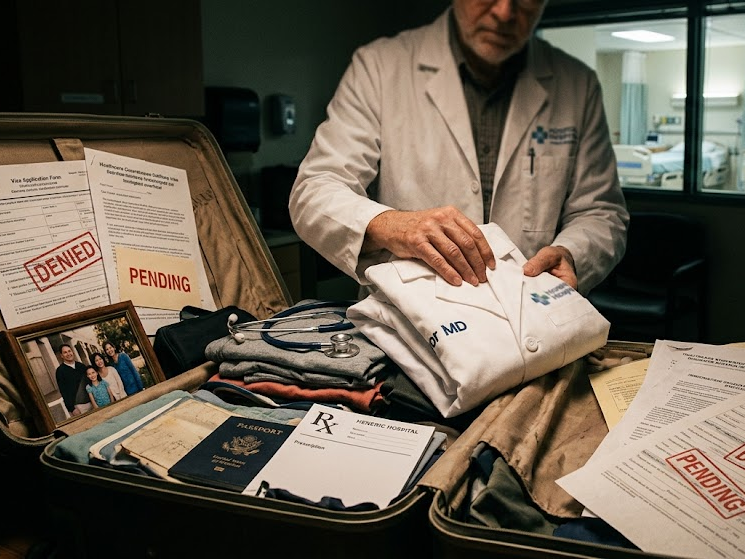
The most devastating and immediate blow to the foreign physician pipeline arrived via a highly controversial Presidential Proclamation.
This executive action was allegedly aimed primarily at prioritizing the hiring of American workers and punishing multinational tech companies for outsourcing practices.
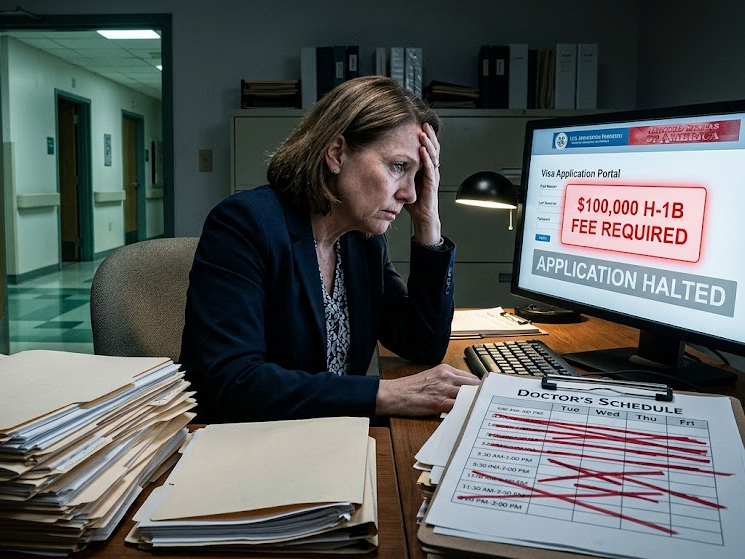
However, the action imposed a massive new financial hurdle that has devastated the medical field: a mandatory, one-time fee of one hundred thousand dollars for all new H-1B visa petitions.
The H-1B visa is a highly specific temporary skilled worker visa that is absolutely critical to the daily functioning of the U.S. healthcare sector.
Hospitals utilize these H-1B visas every single year to legally hire fresh medical residents, specialized fellows, and fully trained attending physicians.
Unlike many other temporary work visas, the H-1B allows for what is known as dual intent.
This means a foreign doctor can legally work and treat patients while simultaneously applying for permanent residency, making it an incredibly crucial tool for the long-term retention of top-tier medical talent.
While this staggering six-figure fee may have been drafted with Silicon Valley tech giants in mind, the healthcare industry was tragically caught directly in the crossfire.
The healthcare sector historically accounts for roughly five percent of all H-1B petitions, yet it relies on these specific visas to fill highly specialized, life-saving, and irreplaceable roles.
For local hospitals, especially non-profit regional health systems and small rural clinics operating on razor-thin financial margins, this massive new fee is simply insurmountable.
Sponsoring just a small cohort of five new foreign-trained medical residents now legally requires half a million dollars in non-refundable visa fees alone.
This extreme financial burden is entirely separate from the actual salaries, benefits, or extensive training costs required to employ these doctors.
Unable to afford these exorbitant and unexpected costs, a massive number of residency programs and independent hospital systems are being aggressively forced to alter their entire recruitment strategies.
Many facilities have entirely abandoned interviewing highly qualified international candidates because they simply do not have the capital to legally hire them.
Red Tape, J-1 Visas, and Sidelined Talent
While the astronomical H-1B fee has effectively choked off the hiring of new foreign medical graduates, additional layers of bureaucratic hurdles are aggressively sidelining the foreign doctors who are already living and working here.
Many IMGs initially enter the U.S. medical training system on J-1 exchange visitor visas.
These specific visas are typically sponsored by the Educational Commission for Foreign Medical Graduates to allow doctors to complete their U.S. residencies.
The current political administration has suddenly implemented drastically enhanced, highly aggressive vetting procedures for these specific visas.
These new rules include extensive reviews of the applicant’s online presence and deep dives into their social media history, ostensibly designed to screen for national security interests.
Recently, the State Department even went so far as to temporarily pause the entire J-1 application processing system, creating an immediate crisis for teaching hospitals.
When the system finally reopened, the intensified scrutiny and new regulations led to massive, insurmountable processing backlogs that have crippled the pipeline.
The situation was further heavily compounded when U.S. Citizenship and Immigration Services suddenly froze automatic extensions of employment authorizations.
They also completely halted vital visa updates for foreign nationals originating from several specifically targeted countries around the globe.
Because medical residencies operate on a highly strict, non-negotiable annual cycle that typically begins in July, these unexpected bureaucratic delays are nothing short of catastrophic.
Physicians who are desperately waiting on backlogged visa renewals are legally prohibited from touching patients or working once their current authorization officially expires.
All across the nation, frantic hospital administrators are reporting that they have been forced to put fully trained, desperately needed foreign physicians on unpaid administrative leave.
These brilliant doctors are quite literally sidelined, forced to sit at home in frustration while hospital waiting rooms overflow with sick patients, simply because the bureaucratic machinery of the immigration system has completely broken down.
Rural America Bears the Heaviest Burden
The devastating collateral damage of these harsh immigration policies falls highly disproportionately on rural America and historically underserved urban neighborhoods.
The traditional, most reliable pathway for many foreign doctors to legally remain in the U.S. after training is the Conrad 30 Waiver program.
Under normal immigration rules, a doctor on a J-1 visa must physically return to their home country for a minimum of two years after completing their U.S. residency before they can ever apply to work in America long-term.
The highly successful Conrad 30 program legally waives this strict requirement if the physician formally agrees to work in a medically underserved American area for three continuous years.
To accomplish this transition, the doctor typically moves from a J-1 training visa to an H-1B working visa.
With the massive new six-figure fee firmly attached to H-1B visas, alongside the extreme administrative delays in processing, this vital rural healthcare pathway is completely breaking down.
Rural clinics and small-town medical boards simply do not have the hundreds of thousands of dollars in surplus capital required to pay a premium just to hire a single physician.
This remains true even if that specific foreign physician is the absolute only cardiologist, pediatrician, or obstetrician willing to relocate to their remote county.
Consequently, the rural areas that often voted heavily for the current political administration are ironically the exact communities bearing the brutal brunt of its strictest immigration policies.
These vulnerable towns are rapidly losing access to the only doctors who have consistently kept their local communities healthy and safe over the past two decades.
How Patient Care is Rapidly Deteriorating
When any administration’s immigration policy sidelines foreign doctors amid a historic medical shortage, the ultimate and most tragic victim is always the everyday American patient.
The basic mathematics of healthcare staffing are brutally unforgiving.
When you abruptly remove thousands of highly trained physicians from the active workforce through sudden visa freezes and prohibitive financial fees, the entire medical system begins to buckle under the pressure.
Everyday patients are already feeling the severe, painful impact of these political decisions.
Wait times to simply establish basic care with a new primary care physician have rapidly stretched from a few weeks to several agonizing months in many parts of the country.
Patients requiring highly specialized medical care, such as advanced endocrinology for diabetes management or complex neurology for stroke recovery, are suffering immensely.
Many of these vulnerable patients are now being forced to drive several hours away from their homes just to reach adequately staffed metropolitan medical centers.
Furthermore, the remaining domestic healthcare workforce is bearing the incredible, crushing brunt of the missing foreign doctors.
Registered nurses, physician assistants, and U.S.-born doctors are constantly being asked to cover exhausting extra shifts and take on dangerously large patient panels just to compensate for the sidelined IMGs.
This directly and aggressively exacerbates the already critical, historic levels of burnout running rampant within the medical profession today.
This extreme burnout leads directly to early, unexpected retirements, which only serves to further shrink the available medical workforce in a terrifying downward spiral.
This vicious, unending cycle of chronic understaffing leads directly to rushed medical appointments, delayed and missed diagnoses, and an overall severe degradation in the fundamental quality of American healthcare.
Industry Backlash and the Demand for Immediate Change
The rapidly escalating crisis has predictably prompted fierce, organized pushback from the entire American medical community.
Major, highly influential industry organizations, including the American Medical Association, the American Hospital Association, and the American Academy of Family Physicians, have sounded the alarm.
These powerful groups are currently actively lobbying the executive branch, lawmakers, and the Department of Homeland Security for immediate, sweeping legislative relief.
Healthcare leaders passionately argue that while strengthening border security and protecting American jobs are valid political priorities, they cannot be applied blindly.
Applying blanket, untargeted immigration restrictions to the highly specialized medical sector is a direct matter of national health security.
The American Medical Association has issued stark, dire warnings that aggressively driving away international medical graduates will directly and undeniably result in American patients suffering and dying.
Medical advocacy groups are currently pushing extremely hard for specific, targeted legal exemptions to these new rules.
They are formally requesting that all medical professionals, clinical researchers, and essential allied health workers be entirely legally exempt from the crippling new visa fees.
Furthermore, these organizations are demanding that immigration agencies immediately reinstate automatic employment extensions for all physicians whose renewals are currently trapped in endless bureaucratic backlogs.
This common-sense fix would instantly allow these vital doctors to remain on the front lines treating sick patients while their paperwork is slowly processed by the government.
Whether the current administration will recognize this crisis, pivot their political stance, and grant these necessary healthcare carve-outs remains entirely to be seen.
However, the medical community insists that the clock is rapidly ticking, and patients are the ones paying the ultimate price.
Conclusion
The vital intersection of federal immigration policy and national healthcare infrastructure is incredibly delicate and complex.
The simple truth is that the United States simply does not produce nearly enough doctors domestically to sustain its vast, rapidly aging population.
For decades, brilliant and dedicated foreign trained physicians have selflessly stepped in to fill this dangerous void.
They have dedicated their lives to healing the sick in some of America’s most isolated, impoverished, and chronically underserved communities.
However, the recent wave of policies emphasizing aggressive enforcement, unprecedented financial visa fees, and intense, delayed vetting have thrown massive wrenches into the gears of the healthcare system.
The terrifying reality that Trump’s immigration policy sidelines foreign doctors amid a shortage is not merely a partisan political talking point.
It is a massive, unfolding public health crisis that is playing out in local emergency rooms, rural clinics, and hospital wards every single day.
Unless federal policymakers quickly recognize the unique, absolutely indispensable role of international medical graduates and implement swift legal exemptions, the consequences will be dire.
The U.S. physician shortage will rapidly evolve from a looming statistical projection into a daily, unavoidable tragedy for millions of American patients seeking basic medical care.
FAQ
Q1. How exactly does the new one hundred thousand dollar H-1B visa fee affect local hospitals and community clinics?
The newly enacted policy legally requires employers to pay a massive, one-time fee to formally sponsor a new H-1B worker visa.
While this policy was allegedly intended to deter massive tech companies from replacing American workers with cheaper foreign labor, it unfortunately applies universally to all industries.
Hospitals, particularly non-profit medical centers and rural health clinics, usually operate on very tight, highly restricted budgets.
Q2. What exactly are J-1 visas, and why are they considered so incredibly important for the U.S. healthcare system?
A J-1 visa is a specific type of exchange visitor visa that is highly commonly used by International Medical Graduates.
They use this visa to legally enter the U.S. in order to complete their required, rigorous medical residency training programs.
It is absolutely critical to the U.S. healthcare system because a massive portion of all primary care and internal medicine residents rely exclusively on it.
Q3. Will the severe doctor shortage caused by these strict immigration policies only negatively affect rural areas?
Absolutely not.
While rural and underserved areas will definitely be hit first and hit the hardest, the negative impacts will quickly ripple throughout the entire country.
Because rural areas rely the most heavily on specific visa waiver programs to recruit physicians, their clinics are the first to lose staff.
However, as the overall national supply of available doctors shrinks, massive urban and wealthy suburban hospitals will also face severe staffing deficits.